Article Text

Abstract
Metabolic dysfunction-associated steatotic liver disease (MASLD) poses a significant global health challenge due to its rising prevalence and strong association with metabolic syndrome and type 2 diabetes mellitus (T2D). Effective management requires a comprehensive approach, emphasising aggressive treatment of obesity and T2D. While lifestyle modifications remain central, anti-diabetic medications such as pioglitazone, glucagon-like peptide-1 receptor agonists, the dual glucagon-like peptide-1 and glucose-dependent insulinotropic polypeptide receptor agonist tirzepatide, and sodium-glucose transporter 2 inhibitors have demonstrated benefits in improving liver parameters and slowing disease progression. These medications not only improve glycaemic control but also reduce hepatic steatosis, liver enzyme levels, and inflammation, with some potential to address fibrosis. Additionally, they offer cardiovascular benefits, which are important for patients with MASLD at heightened cardiovascular risk. However, the histological benefits of metformin and the effects of dipeptidyl peptidase-4 (DPP-4) inhibitors and sulfonylureas remain unclear. Insulin therapy has been shown to reduce hepatic steatosis and improve liver enzyme levels, though its impact on fibrosis is not well documented. A multifaceted treatment strategy targeting metabolic, hepatic and cardiovascular health is essential for effectively managing MASLD and preventing its progression to advanced liver disease.
- HEPATIC FIBROSIS
- FATTY LIVER
- NONALCOHOLIC STEATOHEPATITIS
- LIVER
- CHRONIC LIVER DISEASE
Statistics from Altmetric.com
What is already known on this topic
Metabolic dysfunction-associated steatotic liver disease (MASLD) is strongly associated with type 2 diabetes (T2D) and obesity, increasing the risk of liver fibrosis and cardiovascular disease.
Lifestyle modifications are the cornerstone of MASLD management, but pharmacological interventions using anti-diabetic medications have demonstrated varying levels of efficacy.
What this study adds
This review provides a comprehensive analysis of the effects of various anti-diabetic medications on MASLD, including pioglitazone, GLP-1 receptor agonists, SGLT2 inhibitors and others.
It highlights the multifaceted benefits of these medications, not only in improving glycemic control but also in reducing hepatic steatosis, inflammation and potentially fibrosis.
How this study might affect research, practice or policy
The findings support a personalised, complications-centric approach to MASLD management, emphasising the importance of selecting anti-diabetic medications that offer multisystem benefits.
This review may guide clinicians in optimising treatment strategies for patients with MASLD and T2D, potentially improving liver outcomes, cardiovascular health and overall metabolic profile.
Introduction
Metabolic dysfunction-associated steatotic liver disease (MASLD) is a global health challenge due to its rising prevalence and its close association with metabolic syndrome and type 2 diabetes mellitus (T2D). As the hepatic manifestation of the metabolic syndrome, MASLD is intricately linked to obesity and T2D, both of which exacerbate disease progression and outcomes. Consequently, effective management of MASLD necessitates aggressive treatment of obesity and T2D. While lifestyle modifications remain the cornerstone of MASLD management, pharmacotherapy, particularly the use of anti-diabetic medications, has shown benefits for liver health and disease progression, as well as from extrahepatic causes of morbidity and mortality, especially cardiovascular disease.1 2
MASLD associated with T2D presents the greatest risk for progression to the more severe, necroinflammatory form, metabolic dysfunction-associated steatohepatitis (MASH). T2D is a potent potentiator of fibrogenesis and increases the risk for advanced hepatic fibrosis and hepatocellular carcinoma.3–5 15%–25% of individuals with T2D have clinically significant liver fibrosis, characterised histologically as having moderate or more severe fibrosis at stage F2 or higher.4 6–11 Individuals with MASLD face a twofold to threefold higher risk of developing T2D.12 13 Cardiovascular disease is the leading cause of death in patients with either diabetes or MASLD, and especially in those with both conditions, although in patients with stage F2 fibrosis or higher, liver disease emerges as the predominant cause of mortality.13 Timely diagnosis and treatment of MASLD can prevent or slow the progression of liver disease and lower the risk of developing T2D or cardiovascular disease. MASLD, obesity and T2D share common underlying pathophysiological features, such as insulin resistance and lipotoxicity. As a result, it is understandable that anti-diabetic medications have shown benefits in treating steatotic liver disease.14 15 Clinical practice guidance recommends that together with lifestyle, T2D and pre-diabetes treatment should include consideration for pharmacotherapy with the goals of managing hyperglycaemia and obesity, in addition to targeting liver disease and reducing cardiovascular risk.13 16–18
When treating MASLD and MASH, there are four evidence-based therapeutic goals. The first is the resolution of MASH, characterised by the absence or significant reduction of liver inflammation and the elimination of hepatocyte ballooning, without worsening fibrosis. This can be assessed through liver biopsy or estimated by non-invasive tests (ie, blood-based biomarkers or elastography). The second goal targets the regression of MASLD, aiming for measurable decreases in liver fat accumulation, inflammation or fibrosis. Third, preventing fibrosis progression is crucial, as advanced fibrosis significantly heightens the risk of severe liver complications and liver-related mortality. Advanced fibrosis (stage F3–F4) is a strong predictor of poor outcomes in MASH.19 20 The fourth goal extends beyond liver health to reduce cardiometabolic mortality in patients with MASLD, acknowledging the strong link between liver health and cardiovascular risk and addressing the patient’s overall health profile. This includes improving related comorbidities, such as obesity, dyslipidaemia, hypertension and T2D. Collectively, these goals underscore the comprehensive nature of MASLD and MASH treatment, emphasising the need for a multifaceted approach that extends beyond liver-specific interventions (table 1).13 15
Evidence-based goals when treating MASLD and MASH
Among the various pharmacological agents used to treat T2D, those shown to improve MASH include the thiazolidinedione pioglitazone, glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and the dual glucagon-like peptide-1 and glucose-dependent insulinotropic polypeptide (GLP-1-GIP) RA tirzepatide. Sodium-glucose transporter 2 (SGLT2) inhibitors and insulin may reduce hepatic steatosis, but there is a lack of histological evidence demonstrating their effectiveness in improving steatohepatitis or fibrosis (table 2). Additionally, these medications provide cardiovascular benefits, which are crucial given the heightened risk of cardiovascular disease in patients with MASLD.13 15 21 This review aims to discuss the role of anti-diabetic medications in the management of MASLD, evaluating their effectiveness and risk–benefit profile as treatment options for improving liver outcomes including decreasing hepatic steatosis, liver enzyme levels, inflammation and fibrosis.
Anti-diabetic medications in MASLD and MASH
Pioglitazone
Pioglitazone is a peroxisome proliferator-activated receptor (PPAR) γ agonist used for the treatment of T2D. Pioglitazone’s primary action is to enhance insulin sensitivity, leading to improved glucose and lipid metabolism, which includes reductions in glucose, A1c, and free fatty acid levels. It also ameliorates atherogenic dyslipidaemia by lowering triglycerides, decreasing small dense low-density lipoprotein (LDL) cholesterol, and increasing high-density lipoprotein cholesterol. Additionally, pioglitazone increases adiponectin levels, which correlates with a reduction in visceral fat and improved insulin sensitivity. These effects are believed to contribute to the reversal of MASH.15 22 23 Pioglitazone helps prevent the progression from pre-diabetes to T2D22 and reduces the risk of cardiovascular disease for individuals, whether or not they have diabetes.24–29 The 2023 American Diabetes Association Standards of Care and 2023 American Association of Clinical Endocrinology (AACE) Comprehensive Type 2 Diabetes Management Algorithm recommend the use of pioglitazone to lower the risk of cerebrovascular events and myocardial infarction in patients with diabetes, insulin resistance and a history of stroke.17 30
Pioglitazone may cause dose-dependent weight gain averaging 1%–2% with 15 mg/day and 3%–5% with 45 mg/day.15 23 However, combination therapy with a GLP-1 RA31 32 or SGLT2 inhibitor33–35 results in weight loss. Pioglitazone can cause fluid retention and may cause lower extremity oedema, especially at higher doses or when combined with insulin or amlodipine.13 15 Although pioglitazone has been shown to improve left ventricular diastolic function and reduce epicardial fat,36 37 it can promote heart failure if prescribed to patients with pre-existing heart failure. Pioglitazone should be avoided in individuals with symptomatic heart failure and is contraindicated in those with New York Heart Association Class III and IV heart failure, as it can lead to decompensation of heart failure.13 38
Pioglitazone has been associated with a dose and time-dependent increased risk of bone loss, osteoporosis and fractures, as it can lead to decreased bone mineral density, particularly in postmenopausal women.39 Pioglitazone treatment of patients with pre-diabetes or T2D and MASH for up to 3 years was associated with decreased bone density at the level of the lumbar spine.40 Although some studies have reported no increased fracture risk.41 A baseline bone density measurement is recommended for individuals at higher fracture risk.13 15 Vitamin D and calcium supplementation may prevent bone loss with pioglitazone use in patients with MASH.15 Pioglitazone’s association with bladder cancer remains controversial.23 24 Although current evidence does not support a relationship,25 42 guidelines recommend against its use in active bladder cancer and assessment for microscopic haematuria should be considered prior to initiation.43 However, usage of pioglitazone in the UK is low in routine care. A 2022 analysis found that pioglitazone prescriptions in the UK fell by 24% following bladder cancer safety advisories issued in July 2011.44 Pioglitazone has been recommended for the treatment of MASH in the UK for those with T2D, including a contingency for off-licence use for those without T2D according to the National Institute of Clinical Excellence including in combination with or without vitamin E (1.4.1 In secondary or tertiary care settings only, consider pioglitazone or vitamin E for adults with advanced liver fibrosis, whether they have diabetes or not).45
Pioglitazone in MASLD
Pioglitazone was the first anti-diabetic medication demonstrated in a randomised controlled trial (RCT) to reverse MASH.46 Since that initial finding, there have been several additional RCTs with liver histology as the primary outcome that have compared pioglitazone to placebo for the treatment of MASH in patients with T2D or pre-diabetes.47–51 These studies have consistently shown that pioglitazone can improve key liver histological features, such as steatosis, inflammation, and hepatocellular ballooning, although its effects on fibrosis have been less consistent.13 15 A meta-analysis assessed the use of TZDs in eight RCTs (five with pioglitazone and three with rosiglitazone) in 516 patients with biopsy-proven MASH for a duration of 6–24 months. Among all studies combined, pioglitazone, but not rosiglitazone, was associated with improved advanced fibrosis, fibrosis of any stage, and MASH resolution. The improvement in advanced fibrosis with OR of 3.15 (95% CI 1.25 to 7.93; p=0.01) had a wide CI indicating considerable uncertainty around the true effect size, despite the statistically significant result. Improvement in fibrosis of any stage with OR 1.66 (95% CI 1.12 to 2.47; p=0.01) and NASH resolution with OR 3.22 (95% CI 2.17 to 4.79; p<0.001) had narrower CIs, suggesting more precision in these findings.52
A more recent meta-analysis found that pioglitazone can significantly improve insulin sensitivity, reduce fasting blood glucose and A1c levels, and improve liver enzymes, and histology. However, because the intervention periods in these studies were relatively short, long-term research is still necessary to confirm its efficacy and safety.53 Notably, these trials indicated that pioglitazone doses of 30–45 mg/day led to improvements in MASH. However, improvements in dysglycaemia and dyslipidaemia, along with minimal weight gain, have been observed with a 15 mg/day dose of pioglitazone, which is currently under investigation for MASH.15 Pioglitazone is a cost-effective option for managing patients with both T2D and MASLD. Its affordability, combined with its proven efficacy in addressing both conditions, makes it an especially appealing choice. Nevertheless, there is keen interest in PPAR agonism as a therapeutic target of interest, particularly with the evolution of more specific agonists, as well as additional targeting of additional PPAR-receptor moieties. This includes the development of a deuterium-stabilised enantiomer of pioglitazone (PXL065)54 and pan-PPAR agonists (eg, lanifibranor),55 which in addition to improvements in MASH outcomes, also retain the glycaemic and lipid effects, while also improving cardiovascular outcomes.56
Glucagon-like peptide-1 receptor agonists
GLP-1 RAs mimic the actions of incretin hormones, which are essential for managing T2D and obesity. The primary types of incretin-based therapies include GLP-1 RAs and the dual GLP-1-GIP RA, tirzepatide (table 3). GLP-1 RAs function by stimulating insulin secretion from pancreatic beta cells and inhibiting glucagon release from alpha cells. This increases hepatic glucose uptake and decreases hepatic glucose production, lowering glucose and reducing hepatic de novo lipogenesis. Additionally, these medications slow gastric emptying, enhance satiety and directly affect appetite centres in the brain to decrease appetite and cravings, thereby promoting weight loss.57–59
GLP-1 medications available in the UK
GLP-1 agonism has beneficial effects on lipid metabolism, particularly in reducing hepatic lipid levels through both direct and indirect mechanisms involving the brain, pancreas, liver and gut. In the brain, there is a direct effect on the hypothalamus to suppress appetite, leading to weight loss and a subsequent reduction in liver lipids. In the pancreas, enhanced insulin secretion facilitates the uptake of glucose and fatty acids into adipocytes rather than the liver. Additionally, decreased glucagon secretion leads to reduced hepatic glucose and triglyceride production. Although enterocytes, like hepatocytes, do not express GLP-1 receptors, GLP-1 action is tied to decreased gut chylomicron synthesis and secretion, and decreased gut motility. This results in decreased delivery of lipid substrate to the liver via the gut. GLP-1 directly modulates lipid metabolism in hepatic tissue by downregulating the expression of genes related to lipid metabolism, decreasing secretion of triglycerides and very low-density lipoprotein (VLDL). Collectively, GLP-1 receptor agonism has effects that improve lipid homeostasis by lowering circulating levels of triglycerides and VLDL, reducing the risk of metabolic and cardiovascular complications in patients with MASLD.58 RCTs have shown that GLP-1 RAs can significantly reduce the risk of major adverse cardiovascular events, heart failure with preserved ejection fraction, stroke and cardiovascular death, even in those with the highest CV risk.57 58 60 61 In addition to weight loss and glycaemic control, proposed mechanisms for these cardiovascular benefits include reduced blood pressure, inflammation, postprandial lipaemia and platelet aggregation.57 58 60 61 GLP-1 RA also have established benefits in reducing chronic kidney disease (CKD), reducing albumin excretion and the rate of decline of GFR in patients with T2D (figure 1).57

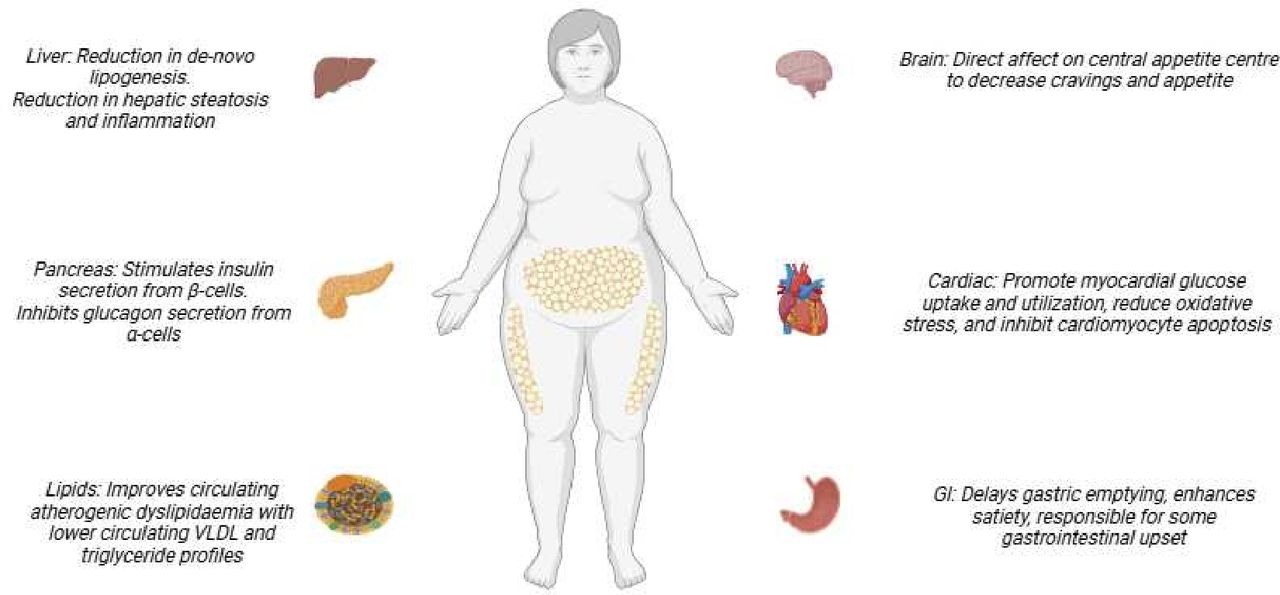{kind=link}
Multisystemic pleiotropic effects of GLP-1 receptor agonism in treatment of MASLD and MASH. This is an original figure created by the authors with the assistance of artificial intelligence. GLP-1, glucagon-like peptide-1; GI, gastrointestinal; MASH, metabolic dysfunction-associated steatohepatitis; MASLD, metabolic dysfunction-associated steatotic liver disease; VLDL, very low-density lipoprotein.
GLP-1 medications have an excellent safety profile and minimal hypoglycaemia. Gastrointestinal side effects (such as nausea, constipation, bloating, diarrhoea and heartburn) are common, occurring in 40%–65% of patients. Vomiting is less common. These side effects are usually transitory but may recur with dose escalation. Importantly, gallbladder events (cholecystitis, cholelithiasis and biliary obstruction sometimes requiring cholecystectomy) occur in up to 3% of patients. Acute kidney injury was reported in <1% of patients, associated with severe nausea, vomiting and dehydration. Decreased gut motility leading to retained gastric contents and aspiration associated with pneumonia is a rare complication, and a consideration for patients who require general anaesthesia. GLP-1 RAs may potentially increase the risk of sarcopenia by affecting muscle mass and function, although evidence remains conflicting and further research is needed to fully understand this relationship. To help prevent muscle loss, consistent resistance exercises and adequate protein intake (1.2–1.6 g/kg of body weight per day) are recommended. GLP-1 medications are associated with a slight increase in heart rate due to their direct action on the sinoatrial node, although in some patients the effect is more substantial. This necessitates careful monitoring in patients with pre-existing cardiovascular disease. Neuropsychiatric events and sarcopenia have also been reported as rare complications. Medullary thyroid carcinoma, pancreatitis and retinopathy are possible complications but have not been conclusively proven to be associated with the use of GLP-1 medications.30 57
GLP-1 RAs in MASLD
The effects of GLP-1 on the liver are indirect, as hepatocytes, Kupffer cells and stellate cells do not express GLP-1 receptors.58 62 In some human studies, circulating levels of endogenous GLP-1 are reduced in patients with MASLD.58 Animal studies and human trials have shown that GLP-1 receptor agonism can reduce hepatic steatosis, inflammation and fibrosis. Weight loss is the primary mechanism for reduction in hepatic steatosis, although the underlying mechanisms for improvements in inflammation and fibrosis are complex and are not yet fully understood.58
RCTs have demonstrated that GLP-1 RAs, such as exenatide, liraglutide and semaglutide, can lead to relative reductions in hepatic steatosis as measured by MRI-based methods.63–67 In a retrospective cohort study of patients with MASLD and T2D, the use of GLP-1 RA was associated with a lower risk of progression to cirrhosis and lower mortality.68 In a phase 2 trial with 320 patients with MASH, including 230 with F2 or F3 fibrosis, semaglutide treatment led to significant MASH resolution without worsening fibrosis compared with placebo.69 72-week data from the Evaluation of Semaglutide in NASH with Enhanced Liver Fibrosis (ESSENCE), a phase 3 trial of semaglutide 2.4 mg weekly, demonstrated statistically significant improvement in both liver fibrosis (37% vs 22.5% on placebo) and MASH resolution (63% vs 34% on placebo).70 A phase 2 trial with semaglutide 2.4 mg weekly was tested in 71 patients with obesity and MASH-related cirrhosis. There was a significant improvement in body weight, liver enzymes, hepatic steatosis, circulating LDL and triglyceride levels. However, there was no significant improvement in MASH resolution or liver fibrosis, likely due to the short 48-week treatment duration and the advanced state of liver disease.71
The dual GLP-1-GIP coagonist tirzepatide enhances the effects of GLP-1 RAs in managing blood sugar levels and weight, and it also seems to offer improvements in the treatment of MASH. Combining GIP receptor agonism with GLP-1 receptor agonism also directly affects white adipose tissue, potentially benefiting patients with MASH.15 The effect of tirzepatide on MASLD was evaluated using MRI-proton density fat fraction in a substudy of the Study of Tirzepatide in Participants with Type 2 Diabetes on Metformin with or without SGLT2 Inhibitor (SURPASS)-3involving 296 patients, which demonstrated significant reductions in subcutaneous and visceral adipose tissue, plasma lipid levels and liver steatosis.72 In the Study of Tirzepatide in Participants With Nonalcoholic Steatohepatitis (SYNERGY-NASH), a 52-week phase 2 RCT involving 157 patients with biopsy-confirmed MASH and stage F2 or F3 fibrosis, tirzepatide was found to be more effective than placebo in resolving MASH without worsening fibrosis, with 62% MASH resolution in the high-dose group compared with 10% in the placebo group. Tirzepatide treatment led to improvements in steatosis, lobular inflammation, hepatocellular ballooning, and changes in fibrosis. Additionally, there were observed changes in body weight, liver enzymes, biomarkers of liver fat, inflammation and fibrosis. 51% of patients in the high-dose tirzepatide group showed improvement in at least one fibrosis stage compared with 30% in the placebo group.21 Although semaglutide and tirzepatide have demonstrated benefits in MASLD, direct comparisons of their liver-specific outcomes are currently lacking. Without head-to-head studies, it is not possible to definitively recommend one over the other based solely on their effects on liver health. While beyond the scope of this article, there is enormous interest in the development of GLP-1 receptor analogues in the MASH arena, which often additionally target other pleiotropic receptors including GIP and glucagon receptor. The majority of these remain in phase II trials and include survovutide,73 retatrutide74 and pemvidutide.75
In summary, GLP-1 RAs provide liver-related benefits for patients with MASLD, including reductions in hepatic steatosis and inflammation, improvements in liver enzyme levels and biomarkers, all of which complement their established benefits in T2D management, weight loss and cardiovascular risk reduction; however, their impact on liver fibrosis has not yet been conclusively demonstrated. The advent of GLP-1 RAs with additional agonism offers theoretical benefits over GLP-1 RAs alone and is an ongoing area of intense interest.
SGLT2 inhibitors
SGLT2 inhibitors have become the standard of care for managing T2D, heart failure and CKD. SGLTs are a family of proteins that facilitate the active transport of glucose across cell membranes. SGLTs function as cotransporters, coupling the transport of glucose with sodium ions. In the kidney, SGLTs facilitate the reabsorption of glucose from the urine back into the bloodstream. SGLT2 inhibitors block this process, promoting the excretion of glucose through urine, thereby reducing blood sugar levels.76 In addition to treating diabetes, SGLT2 inhibitors have been shown to reduce cardiovascular events and improve renal outcomes in patients with CKD, whether they have diabetes or not. These medications also possess a diuretic effect, which helps lower blood pressure and manage fluid overload, thereby supporting their protective benefits for the heart and kidneys.17 30 77 78 By decreasing glucotoxicity, SGLT2 inhibitors enhance β-cell function and contribute to improved insulin sensitivity.79
Studies have consistently shown that SGLT2 inhibitors lead to weight loss in patients with T2D, with similar outcomes observed across various agents and dosages. In the Canagliflozin cardioVascular Assessment Study (CANVAS), patients with T2D and high cardiovascular risk treated with canagliflozin had an average weight loss of about 2–4 kg compared with placebo.80 Trials with dapagliflozin and ertugliflozin demonstrated a mean weight loss of 2–3 kg compared with placebo.81 82 A meta-analysis of 551 patients treated with SGLT2 inhibitors found a mean weight loss of −1.8 kg and −2.4 kg.83 SGLT2 inhibitors primarily facilitate weight loss by inducing glycosuria, which leads to caloric loss through the excretion of glucose in urine. SGLT2 inhibitors may also contribute to weight loss by promoting lipolysis in adipose tissue and depleting glycogen stores in the liver.84
SGLT2 inhibitors are generally well tolerated and adverse effects are typically mild. The predominant risk of SGLT2 inhibitors is the association with genitourinary tract infections, suspected to be secondary to the increase in glycosuria.85 86 Due to their osmotic diuretic effect, SGLT2 inhibitors can cause polyuria, dehydration and orthostatic hypotension. There is a potential risk of acute kidney injury, especially if the patient is taking other medications that affect kidney function. Fournier’s gangrene, a rare necrotising infection affecting the genital, perineal and perianal regions, has been identified as a serious but uncommon adverse event associated with SGLT2 inhibitors.87 88 However, two large studies found no statistically significant link between SGLT2 inhibitors and Fournier’s gangrene, casting doubt on the purported increased risk.89 90
Another significant side effect infrequently associated with SGLT2 inhibitors is the risk of diabetic ketoacidosis (DKA). Typically, SGLT2 inhibitor-related DKA presents as euglycaemic or with mild hyperglycaemia, with glucose levels frequently below 200 mg/dL. However, a recent meta-analysis found no increased risk of DKA associated with the use of SGLT2 inhibitors.91 A potential link between SGLT2 inhibitors and an increased risk of amputations and fractures was initially observed, primarily in the CANVAS programme. However, this relationship has not been supported by meta-analyses.80 92
SGLT2 inhibitors in MASLD
SGLT2 inhibitors have been shown to decrease hepatic steatosis in RCTs with non-invasive tests, primarily MRI-based methods.93–100 Currently, there are no RCTs assessing liver histology outcomes with SGLT2 inhibitors. Reduction in hepatic steatosis has been seen with dapagliflozin,96 empagliflozin97–99 and canagliflozin.95 In a RCT, participants with MASLD who received empagliflozin for 24 weeks experienced a significant reduction in liver stiffness, an indirect measure of liver fibrosis, evaluated by transient elastography, compared with those in the placebo group.101 A 24-week randomised controlled trial comparing empagliflozin with pioglitazone and placebo found that empagliflozin significantly reduced liver stiffness, as measured by transient elastography, compared with both pioglitazone and placebo.102 RCTs with paired biopsies are needed to understand the full effect of SGLT2 inhibitors in MASLD and MASH.15 Although the evidence for SGLT2 inhibitors in MASLD is limited, guidelines recommend that they can be used as an additional treatment for people with T2D and MASLD, as they help reduce hepatic steatosis and provide considerable cardiometabolic and kidney protection.13
Other anti-diabetic medications and MASLD
Metformin use in patients with MASLD leads to improvements in liver enzymes and insulin resistance; however, these benefits are likely attributable to the reductions in body weight. Metformin does not result in significant histological changes. A pilot study in 28 patients with paired liver biopsies assessing the effect of metformin for the treatment of MASH found that metformin led to improvements in liver histology and ALT levels in 30% of patients.103 An open-label trial of metformin in patients with MASLD without diabetes found significant reductions in ALT levels and hepatic steatosis and non-significant decreases in necroinflammation and fibrosis were observed through liver biopsy.104 A systematic review and meta-analysis on the use of metformin in MASLD found improvements in liver enzymes, insulin resistance and BMI; however, there was no significant histological response, with no notable differences in steatosis, inflammation, hepatocellular ballooning or fibrosis.105 Although metformin is not recommended for the treatment of MASLD because it has shown no benefit for liver-related outcomes, it may be used as needed for the treatment of hyperglycaemia in patients with T2D.13 Although DPP-4 inhibitors have been shown to improve liver steatosis, inflammation and fibrosis in animal models, RCTs have not found that DDP-4 inhibitors reduce hepatic steatosis or fibrosis in patients with T2D or pre-diabetes.106–108 The impact of sulfonylureas on MASLD has not been well-established.13 Insulin therapy positively impacts MASLD by reducing hepatic steatosis and improving liver enzyme levels.109–111 An RCT comparing insulin glargine to liraglutide found that both treatments similarly decreased MRI-based measures of liver fat content.112 However, the effect of insulin on MASH and liver fibrosis has not been well documented (table 2).13
Conclusion
The management of MASLD requires a comprehensive approach that recognises its strong association with insulin resistance, metabolic syndrome and T2D. Screening for advanced liver fibrosis should begin at the primary care level, where less complex cases are typically managed. Primary care physicians play a vital role in initial assessment, lifestyle counselling and prescribing anti-diabetic medications. They also coordinate care and monitor disease progression. More complex cases are referred to specialists, with endocrinologists managing advanced metabolic complications and hepatologists addressing severe liver issues. This tiered approach ensures efficient use of resources while providing comprehensive care. Effective management relies on clear communication channels between primary care and specialists, shared electronic records and standardised care pathways. This integrated model allows for coordinated treatment of MASLD and its associated comorbidities, tailoring interventions to each patient’s specific needs. While lifestyle modifications remain fundamental, the integration of anti-diabetic pharmacotherapy offers additional benefits for MASLD. These medications can be vital in early disease management, maximising time-sensitive opportunities for reversal and delayed progression of MASLD. Pioglitazone, GLP-1 RAs, tirzepatide and SGLT2 inhibitors not only improve glycaemic control but also contribute to reductions in hepatic steatosis, liver enzyme levels and inflammation, with some showing potential in addressing fibrosis. This review highlights the continued importance of pioglitazone in managing MASLD and T2D, emphasising its potential synergistic effects when combined with GLP-1 RAs for patients with MASLD fibrosis. The cardiovascular benefits of these medications are an additional benefit given the high associated mortality. Insulin reduces hepatic steatosis and liver enzymes but does not have histological data. There are no histological benefits of metformin and limited data for DPP-4 inhibitors and sulfonylureas.
The management of patients with MASLD and T2D requires a personalised, comprehensive approach. A complications-centric strategy is essential, considering the patient’s overall metabolic profile, cardiovascular risk, renal function and weight. When selecting antidiabetic medications, clinicians should prioritise agents that offer multisystem benefits. For instance, GLP-1 RAs and tirzepatide have demonstrated advantages in reduction of hepatic steatosis and fibrosis, weight loss and cardiovascular protection, whereas SGLT2 inhibitors have demonstrated cardiovascular and renal benefits. Pioglitazone, while effective for liver health and glycaemic control, may be particularly suitable for patients with a history of cardiovascular disease, especially stroke or where cost is an issue. The choice and sequence of medications should be tailored to each patient’s specific needs, comorbidities and risk factors, aiming to optimise not only liver outcomes but also overall metabolic health, cardiovascular protection and renal function. Ideally, a multifaceted treatment strategy that targets metabolic, hepatic and cardiovascular health is essential for effectively managing MASLD and preventing its progression to advanced liver disease. Continued research and clinical trials are necessary for harmonising ideal therapeutic approaches and improving outcomes for patients with T2D and MASLD.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
X @scottisaacsmd, @brennap9
Contributors SI contributed substantially to the conception and design of the work, conducted comprehensive literature reviews, performed data analysis and interpretation, drafted significant portions of the manuscript, and created tables. FF performed data analysis and interpretation and drafted significant portions of the manuscript. PNB made substantial contributions to the writing of the manuscript, conducted supplemental literature searches, participated in data analysis and interpretation, and created the figure. All authors were involved in critically revising the work for important intellectual content, gave final approval of the version to be published, and agree to be accountable for all aspects of the work. All individuals named in this contributorship statement gave permission to be included. SI serves as the guarantor for this study, accepting full responsibility for the work and/or the conduct of the study, had access to the data and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.