Article Text

Abstract
Endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) is one of the safest minimally invasive modalities for tissue acquisition from submucosal lesions in and near the gastrointestinal tract. Rapid on-site cytologic evaluation (ROSE) is an attempt to improve the efficacy of EUS-FNA. It is a laboratory service that evaluates the cytomorphological features of FNA smears and biopsy touch imprints to offer real-time feedback and guidance during biopsy. The current systematic review compares the effectiveness of ROSE to macroscopic on-site evaluation (MOSE), focusing on cost, diagnostic accuracy and sensitivity, likelihood of adverse effects and procedure duration. The present systematic review is written following the regulations recommended by the Cochrane and Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The databases searched were Cochrane CENTRAL, PubMed and Google Scholar. 16 studies met the inclusion criteria and were selected for this review. The findings established that ROSE aids in the improvement of diagnostic yield during FNA or biopsy procedures. However, it is time consuming, putting pressure on an institution’s resources. The systematic review also established that the ROSE significantly enhances the EUS-FNA procedure. The findings indicated that MOSE reduced procedure time, required fewer needle passes and could be easily accessed. MOSE+fine-needle biopsy demonstrated a shorter procedure time. MOSE is more effective than ROSE due to its accessibility, and fewer needle passes are needed to establish a diagnosis. However, the findings show that MOSE and ROSE display similar diagnostic yield, accuracy, sensitivity and specificity.
- CHRONIC PANCREATITIS
- ENDOSCOPIC PROCEDURES
- ENDOSCOPIC ULTRASONOGRAPHY
- HEPATOBILIARY DISEASE
- LIVER BIOPSY
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- CHRONIC PANCREATITIS
- ENDOSCOPIC PROCEDURES
- ENDOSCOPIC ULTRASONOGRAPHY
- HEPATOBILIARY DISEASE
- LIVER BIOPSY
WHAT IS ALREADY KNOWN ON THIS TOPIC
Endoscopic ultrasound (EUS)-guided fine-needle aspiration is a safe and effective method for tissue acquisition with high diagnostic sensitivity, but rapid on-site cytologic evaluation (ROSE), while enhancing diagnostic yield, is time consuming and often inaccessible in community settings.
There was a lack of systematic reviews comparing ROSE and macroscopic on-site evaluation (MOSE) regarding their effectiveness, efficiency and cost-effectiveness.
WHAT THIS STUDY ADDS
The study provides evidence that MOSE is more efficient and cost-effective than ROSE, requiring fewer needle passes and shorter procedure times while maintaining similar diagnostic accuracy.
The study highlights how MOSE can enhance patient care and optimise resource allocation, especially in settings with limited access to cytopathologists.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The findings encourage the adoption of MOSE in EUS-guided procedures, potentially improving patient outcomes and procedural efficiency.
Healthcare policies may be influenced to standardise the use of MOSE in tissue acquisition practices, particularly in community healthcare environments.
Background
Endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) is one of the safest minimally invasive modalities for tissue acquisition from submucosal lesions in and near the gastrointestinal (GI) tract.1 It has high diagnostic sensitivity and accuracy, making it the recommended first-line modality for tissue acquisition in patients with suspected malignancies and tumours.2 However, EUS-guided specimen sampling is one of the most challenging tissue acquisition procedures. Consequently, proper techniques, accessories and on-site cytopathology evaluation are essential to maximising the diagnostic yield. Rapid on-site cytologic evaluation (ROSE) is an attempt to improve the efficacy of EUS-FNA.3 ROSE has been instrumental in improving the diagnostic yield of biopsy procedures and acquiring sufficient specimens for auxiliary testing.4 However, ROSE is inaccessible outside tertiary centres, especially in community healthcare centres, due to the complexity of expertise development and costs.5 Macroscopic on-site evaluation (MOSE) is comparable to ROSE when used with EUS core tissue biopsy needles.6
ROSE is undertaken during EUS-FNA to assess each pass’s sufficiency and triage the acquired specimen to other cases and studies. During ROSE, the cytopathologist microscopically scrutinises the prepared slide in real time to determine whether the aspirated material is adequate. The procedure is stopped if the acquired specimen is sufficient.7 In contrast, if there is necrosis or no material, the endoscopist can adjust the needle to another part of the lesion. Consequently, ROSE refines EUS-FNA by minimising the number of insufficient diagnoses while reducing the number of passes.8 Nevertheless, the practical use of ROSE is limited due to cost, which makes some pathologists fail to offer it.
Conversely, MOSE is the on-site evaluation technique used for EUS-guided fine-needle biopsy (EUS-FNB), whose results in acquiring larger tissue pieces enable histological diagnosis, eliminating the need for ROSE.9 Therefore, during EUS-FNB, endoscopists undertake MOSE to establish whether the specimen is adequate or if other passes are necessary. MOSE with EUS-FNB eliminates the need for on-site cytopathologists, making MOSE relatively more affordable. According to Chen et al,10 EUS-FNB with MOSE is preferable to EUS-FNA with ROSE because it requires fewer needle passes and shorter procedure time and offers fewer adverse effects without reducing diagnostic accuracy.
Based on the evidence above, selecting the most effective tissue acquisition depends on various factors, for example, preferred specimen type, molecular test and cytopathologist preferences. Therefore, there is an overarching need for adequate training and experience to optimise the accuracy and safety of EUS-guided procedures. Appreciating the fundamentals of these EUS techniques enables appropriate patient management before, after and during the procedure. Therefore, it is necessary to compare ROSE and MOSE to determine the best alternative for acquiring specimens from the lesions, lymphomas and tumours. The current systematic review aims to compare the effectiveness of ROSE to MOSE, focusing on cost, diagnostic accuracy and sensitivity, likelihood of adverse effects and procedure duration.
Methodology
Study design
The present systematic review complies with the regulations recommended by the Cochrane methodology. Further, the reporting procedure followed in the review abides by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).11
Literature search
A comprehensive online search was performed to find articles for the current systematic review. The search strategies were leveraged across three primary electronic databases, that is, Google Scholar, PubMed and Cochrane Central. Additionally, more pertinent studies were revealed by skimming through the reference pages of systematic reviews and meta-analyses focusing on the comparative analyses of ROSE and MOSE. The systematic review included all published studies from its inception to January 2025. A more advanced electronic search was undertaken on the aforementioned databases with the aid of key terms, namely MeSH terms (Medical Subject Headings), Boolean operators (OR and AND), truncations and field tags, which narrowed the focus of the research. Advanced search techniques were collaboratively leveraged to design a conceptual search string to help with the search. The conceptual search string used in the study was: (rapid on-site evaluation OR rapid on-site cytologic evaluation OR ROSE) AND (macroscopic on-site evaluation OR MOSE) AND (lesions).
Eligibility criteria
The inclusion and exclusion criteria for the systematic review were based on the Patient/Population, intervention, comparison and outcomes (PICO) framework. This systematic review only included articles whose subjects were patients with lesions in the GI or the neighbouring organs like the pancreas, lung and lymph nodes. The lesions could be from cell tumours, lymphomas or metastatic cancers. Besides, the present systematic review only included articles where the tissue acquisition strategies used were EUS guided, with their efficiencies improved through either ROSE or MOSE. The controls for the relevant papers were EUS-FNA without MOSE or ROSE. Therefore, any article that utilised a different method for tissue acquisition was omitted. The articles in the systematic reviews focused on various outcomes of the ROSE or MOSE, including diagnostic accuracy, sensitivity, number of needles and passes used, cost, adverse effects and procedure duration. The articles which did not address any of the outcomes were excluded.
Screening and data selection
First, the screening was initiated by eliminating duplicates from the three databases. Next, the remaining articles were screened based on their titles, as they revealed which articles were pertinent to the systematic review. After eliminating studies based on their titles, the remaining articles were selected based on the content of the abstracts. The articles established to be irrelevant based on their abstracts were eliminated. After that, the remaining articles were screened based on carefully reviewing their full texts. The full-text screening of the remaining articles was performed based on the PICO framework as discussed in the eligibility criteria. The peer-reviewed articles that passed the rigorous screening process were intensely scrutinised, and the relevant information was extracted to support the systematic review’s conclusions.
Quality assessment
Two reviewers conducted quality evaluation according to the study type assessed. The Risk-Of-Bias (ROB)-2 tool was used to analyse the quality of the randomised controlled trials (RCT).12 The tool evaluated five domains for each study: (D1) bias due to randomisation, (D2) bias as a result of deviations from intended intervention, (D3) bias due to data missing, (D4) bias due to results and (D5) bias due to selection of reported outcome. The domains were either judged as ‘High’, ‘Low’ or ‘Some concern’. On the other hand, the Newcastle-Ottawa Scale was used to analyse the quality of retrospective and prospective cohort studies. The scale consists of three sections: comparability, selection and outcome. The overall score ranges from 0 to 9, with higher scores (≥7) showing high-quality, moderate scores (4–6) signifying fair quality, and lower scores (0–3) indicating the low quality of the studies.13
Data extraction
The data mined from the peer-reviewed articles in the present systematic review were organised in a preset comma-separated value (CVS) document, preferably a Microsoft Excel spreadsheet. The Excel spreadsheet has columns for the authors (year of publication), study design, participants, intervention, control and outcomes. Then, each article included in the systematic review was organised in the rows of the spreadsheet. After that, the authors independently collected the pertinent data from the included articles. Finally, arising issues and incongruences were resolved through discussions with a third-party consultant.
Results
Study selection
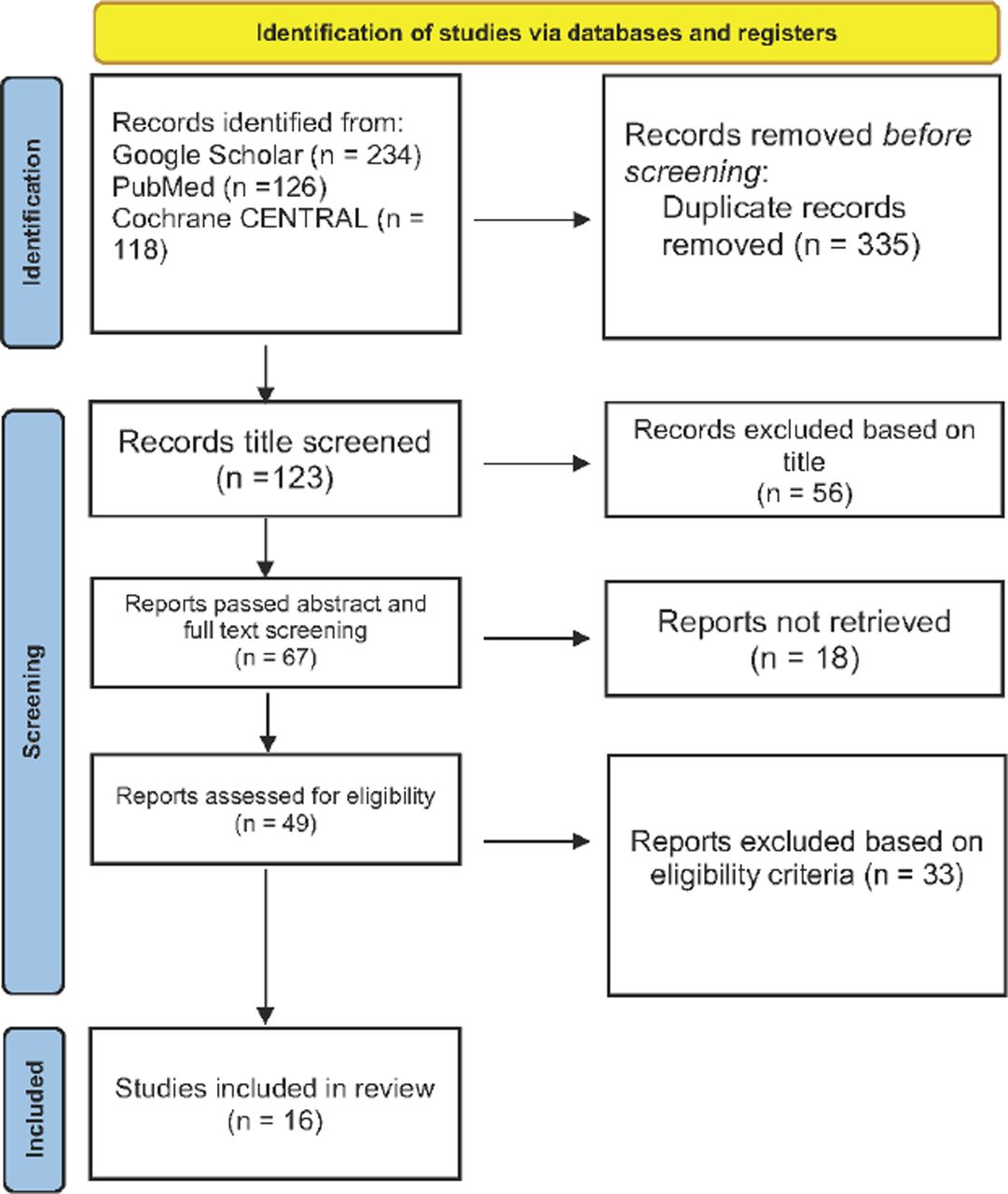
The database searches yielded 478 articles. The elimination of duplicates from the different databases resulted in the exclusion of 355 records, leaving 123 studies that were then screened for relevance based on their titles and abstracts. A thorough perusal of the titles and abstracts eliminated 56 studies, leaving 67 articles for further review. Most eliminated articles did not mention MOSE and ROSE in the titles and abstracts, resulting in a widespread elimination of the articles. The remaining 67 articles were sought for retrieval, resulting in the elimination of 18 articles. These excluded records were not retrieved because of ongoing clinical trials, case reports, editorials, review articles or commentaries. After that, a full-text eligibility criteria scanning of the 49 articles was undertaken, resulting in the elimination of 33 articles as follows: reported irrelevant outcomes (11), did not involve ROSE or MOSE (13) and did not report on patients with lesions (9). Consequently, 16 articles met the inclusion criteria. The study selection for the systematic review is summarised in the PRISMA flow diagram (figure 1).

A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart summarising the identification of studies.
Study characteristics
The systematic review included 16 peer-reviewed articles categorised into six randomised controlled articles,10 14–18 seven retrospective studies6 19–24 and three prospective studies.9 25 26 The 16 articles included a total of 3279 patients with lesions. Besides, the average age of the subjects across all the included studies was above 55 years. The eight articles explored different EUS-guided fine-needle tissue acquisition methods with and without on-site evaluations. Out of the 16 articles, seven studies examined the effect of MOSE on diagnostic accuracy, yield, specificity, sensitivity, procedure time and number of passes.6 9 18 20 21 24 26 Similarly, one article compared the accuracy, sensitivity and specificity of conventional EUS-guided fine-needle tissue acquisition to EUS-guided fine-needle tissue acquisition with MOSE.14 Similarly, seven articles compared the accuracy, specificity and sensitivity of EUS-guided fine-needle tissue acquisition with and without ROSE.10 15–17 19 22 25 The remaining article compared the efficacy of ROSE and MOSE.23 Two studies compared the effectiveness of ROSE in cost minimisation during EUS10 19 (online supplemental table 1).
Supplemental material
Risk of bias and quality assessment
All the studies demonstrated a consistently low risk of bias in all five domains (figure 2). Consequently, all the studies can be deemed of good methodological quality, evidenced by a low risk of bias.

{kind=link}
{kind=link}
Risk of bias summary of the included randomised controlled trials (RCTs).
A summary of the quality appraisal outcomes is shown in online supplemental table 2. We found that all the studies had fair methodological quality from the assessment. All studies did not blind outcome assessors; therefore, no score was provided under the assessment scores.
Discussion
This systematic review found that EUS-FNA coupled with ROSE has a diagnostic accuracy of >90%, consistent with several previous articles.27 28 ROSE aids in the improvement of diagnostic yield during FNA or biopsy procedures. However, ROSE is a time-consuming procedure that pressures an institution’s resources. The systematic review established that the ROSE significantly enhanced the EUS-FNA procedure. Milluzzo et al22 reported that ROSE improved the diagnostic accuracy of the EUS-FNA procedure from 69.2% to 86.2%. Besides, ROSE was shown to significantly improve diagnostic adequacy, yield, specificity and sensitivity.
The review provided the outcomes of the cost minimisation evaluation, comparing EUS-FNA+ROSE versus EUS-FNB.10 Specifically, the study established that EUS-FNB expenses were slightly higher than FNA+ROSE (both in Canada and the USA) but clinically insignificant. These outcomes align with two RCTs that evaluated the cost minimisation analysis comparing EUS-FNA+ROSE and FNA alone in assessing pancreatic masses.29 30 Sbeit and Khoury reported a similar cost minimisation analysis, highlighting no cost-effectiveness of EUS-FNB over EUS-FNA+ROSE.19
Moreover, this review has established that EUS-FNB (with MOSE) requires fewer needle passes to establish diagnosis than FNA despite having comparable diagnostic accuracy and adequacy.18 The findings align with a recent study that annotates that FNB needles need fewer needle passes to determine the diagnosis.31
The fundamental benefits of ROSE vary depending on whether imaging guidance is used or not. The effectiveness of ROSE varies depending on the different organic systems and entities, such as metastatic cancers, lymphomas and submucosal lesions. The high adequacy and yield retrieved through ROSE make it highly effective in specimen triage and sampling adequacy assessment.7 The systematic review determined that when the new-generation biopsy needles were used to evaluate lesions, EUS-FNB with the adequacy assessed through MOSE had the same diagnostic accuracy, specificity and sensitivity as EUS-FNA with ROSE.23 The comparison between MOSE and conventional EUS-FNA (89.3%) revealed that MOSE had a higher diagnostic adequacy (92.6%) with considerably fewer passes. Therefore, MOSE could be leveraged as an alternative to ROSE since it could be used to evaluate the adequacy of sampling without any significant difference in diagnostic accuracy for solid pancreatic lesions (SPL).
The comparison between MOSE and ROSE revealed a need to reconsider the utilisation of ROSE while using core biopsy needles concerning cost and logistics. While ROSE was crucial in optimising the performance of EUS-FNA cytology for SPLs, the emergence of EUS-FNB needs to revolutionise EUS-FNA. EUS-FNB could collect a highly cellular specimen and establish a diagnostic accuracy of >90% on a single pass, eliminating the need for ROSE. MOSE is more effective than ROSE when used with core biopsy needles.23 Consequently, MOSE is considerably more effective due to cost and logistics as it uses significantly lower passes, mainly when used with core biopsy needles.
Limitations
First, most studies focused on the differences between EUS-FNA and EUS-FNB without considering the accompanying techniques and strategies leveraged to improve the procedures’ diagnostic yield, accuracy, sensitivity and specificity. Another major limitation of the current systematic review is the varying outcomes. Some articles focused on accuracy, specificity and sensitivity, while others concentrated on the number of passes, diagnostic yield and procedure duration. The disparity in the outcomes affects the comparison of ROSE and MOSE.
Conclusions
The present systematic review established that MOSE is a more cost-effective evaluation technique than ROSE, mainly used with EUS-FNB. Using EUS-FNB obviated the need for ROSE as it has a high diagnostic yield, accuracy, sensitivity and specificity. The results vouch for the superiority of EUS-FNB alone over EUS-FNA for assessing lesions, suggesting the need to convert to FNB. Additionally, the findings have far-reaching and profound implications as they are likely to revolutionise modern patient care. For clinicians, determining which tissue acquisition techniques are more effective is essential in improving their quality of care. The systematic review’s findings offer insight into how diagnostic methods can be improved by determining the benefits of MOSE over ROSE when using biopsy core needles.
Supplemental material
Supplemental material
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Contributors EG, BM and HO contributed to conceptualisation. SAG, EA, CB, HS, DV, AA and IR contributed to resources, writing, reviewing and editing. EG and HO contributed to supervision and project administration. All authors contributed to and approved of the final draft. EG is responsible for the overall content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.